Lithium
Excerpt from Cafer's Mood Stabilizers and Antiepileptics

Neuroprotectant
FDA approved for:
Used off-label for:
❖ Depression ❖ Suicidal ideation ❖ Dementia ❖ Alcoholism ❖ Agitation
❖ Headaches ❖ Neutropenia ❖ SIADH ❖ Longevity
Lithium is the gold standard treatment for bipolar disorder. It is superior to all medications at preventing suicide, reducing risk 5-fold for individuals with recurrent unipolar depression and 6-fold for those with bipolar disorder (Tondo et al, 2016). It works by several mechanisms that are not entirely understood.

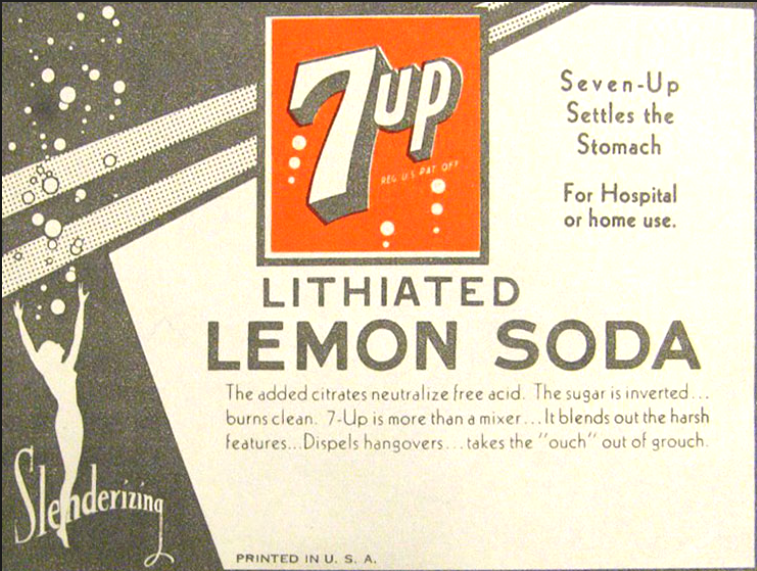
Lithium citrate was added to 7-Up (originally known as Bib-Label Lithiated Lemon-Lime Soda) from 1929–1950. The “7” refers to Lithium’s atomic mass. Prescription lithium is available as lithium citrate syrup but is usually dispensed as lithium carbonate tablets or capsules.
Lithium is an element on the periodic table, classified as an alkali metal. Its atomic number is 3, making it the 3rd lightest element. Lithium was one of the first three elements in existence with the big bang (along with helium and hydrogen) over 13 billion years ago.
Lithium citrate was added to 7-Up (originally known as Bib-Label Lithiated Lemon-Lime Soda) from 1929–1950. The “7” refers to Lithium’s atomic mass. Prescription lithium is available as lithium citrate syrup but is usually dispensed as lithium carbonate tablets or capsules.
FDA approved in 1970, Lithium is the only mood stabilizer that is not an antiepileptic. Antiepileptics raise seizure threshold. Lithium modestly decreases seizure threshold, making seizures slightly more likely to occur.
Lithium is neuroprotective, i.e., keeps neurons from dying. It is arguably an essential trace nutrient for mental wellbeing. Small amounts of lithium are present in vegetables and drinking water. Higher amounts of naturally occurring lithium in drinking water have been associated with decreased rates of suicide and violent crime (GN Schrauzer et al, 1990). Lithium has been shown to extend healthy lifespan of Drosophila fruit flies by about 8% (Castillo-Quan et al, 2016). Long-term exposure to low dose lithium appears to promote longevity in humans (Zarse et al, 2011). Lithium is an effective treatment for Alzheimer’s disease (Mauer et al, 2014) and might prevent pre-dementia from progressing to Alzheimer’s disease (Forlenza et al, 2011). The mechanism of neuroprotection and mood stabilization appears to involve brain-derived neurotrophic factor (BDNF).
Lithium is a first-line add-on for treatment-resistant unipolar depression, usually at a low to moderate dose. 68% of depressed patients over age 65 responded to lithium augmentation, improving faster than younger individuals. 47% of those < 65 responded (Buspavanich et al, 2019). Lithium is used off-label for prevention of migraine, cluster, and vascular headaches. Lithium increases white blood cell (WBC) count, making it a treatment option for neutropenia, including clozapine-induced neutropenia. Lithium inhibits antidiuretic hormone (ADH) and can be used to counter syndrome of inappropriate ADH secretion (SIADH).
Lithium is renally cleared, unmetabolized. As an element, there is nothing it could be metabolized to. Therefore it is not involved in CYP enzyme interactions. Lithium is subject to kinetic interactions when other drugs affect the rate of lithium clearance by the kidneys. Lithium has a narrow therapeutic index, i.e., the toxic range is not far from the therapeutic range. A black box warning advises to start lithium only if a facility is available for prompt serum level testing. Signs of lithium toxicity include tremor, diarrhea, vomiting, abdominal pain, weakness, and sedation. Consequences of lithium toxicity may include renal damage, seizure, and coma.
Although toxic lithium levels can result in cardiac conduction delays, at therapeutic doses lithium is cardioprotective and lowers the risk of myocardial infarction. Lithium does not increase risk of stroke, which cannot be said of carbamazepine (Chen et al, 2019).
To avoid lithium toxicity, patients should be advised to avoid NSAIDS (ibuprofen, naproxen) and instead use aspirin or acetaminophen for pain. Patients should also remind their other doctors that they are on lithium, especially when diuretics or blood pressure medications are discussed. The most significant contributors to lithium toxicity are NSAIDS and thiazide diuretics, including hydrochlorothiazide (HCTZ) and chlorthalidone. See page 26 for the full list of “battery chargers” that increase lithium levels (ACE inhibitors, ARBs, metronidazole, etc).
Lithium side effects are dose-dependent, including weight gain, fine tremor, acne, excessive thirst, and frequent urination. If thirst and polyuria are extreme, the cause may be lithium-induced nephrogenic diabetes insipidus (deficient response by kidneys to ADH). If nausea is a problem, reduce dose or switch to Lithium ER (Lithobid). Otherwise, immediate release lithium is preferable for maintenance treatment. Taking the entire daily dose of immediate release lithium at bedtime reduces polyuria and decreases the risk of renal problems (Gitlin et al, 2016) by giving the kidneys a break.
Lithium increases the incidence of hypothyroidism 6-fold. Since about 15% of lithium-treated patients will become hypothyroid, TSH should be monitored routinely so levothyroxine (Synthroid) can be added if TSH gets high. Renal function needs to be monitored with a metabolic panel (BMP or CMP). When lithium is combined with a 1st generation antipsychotic, extrapyramidal symptoms (EPS) and neuroleptic malignant syndrome (NMS) may be more likely, which is considered a neurotoxic effect of unknown mechanism. Rarely, lithium may contribute to serotonin syndrome. For individuals over age 50, it is recommended to get an EKG prior to starting (standard-dose) lithium because arrhythmias are possible. Very rarely lithium is associated with intracranial hypertension (pseudotumor cerebri), which presents as headache and ringing in the ears with heartbeats. If untreated, intracranial hypertension can lead to loss of vision.
When taken during the first trimester of pregnancy, lithium poses a low risk (1 in 1,500) of Ebstein's anomaly, a cardiac condition involving the tricuspid valve. Lithium is certainly less teratogenic than valproic acid (Depakote, Depakene) or carbamazepine (Tegretol). Lithium is considered safe for fetal development after the first trimester, but maintaining steady lithium levels during pregnancy and after delivery is challenging. Lithium concentration of fetal blood is equal to that of maternal blood with levels continually decreasing in the first and second trimesters, risking subtherapeutic concentration. Lithium concentration gradually increases in the third trimester and in the postpartum, risking toxicity. If lithium is continued during pregnancy, levels should be checked weekly.
In 2019 the FDA lowered the approved minimum age for lithium from 12 to 7 years.
Lithium works well in combination with valproic acid (Depakote, Depakene), lamotrigine (Lamictal), and second-generation antipsychotics (SGAs).
Lithium is renally cleared, unmetabolized. As an element, there is nothing it could be metabolized to. Therefore it is not involved in CYP enzyme interactions. Lithium is subject to kinetic interactions when other drugs affect the rate of lithium clearance by the kidneys. Lithium has a narrow therapeutic index, i.e., the toxic range is not far from the therapeutic range. A black box warning advises to start lithium only if a facility is available for prompt serum level testing. Signs of lithium toxicity include tremor, diarrhea, vomiting, abdominal pain, weakness, and sedation. Consequences of lithium toxicity may include renal damage, seizure, and coma.
Although toxic lithium levels can result in cardiac conduction delays, at therapeutic doses lithium is cardioprotective and lowers the risk of myocardial infarction. Lithium does not increase risk of stroke, which cannot be said of carbamazepine (Chen et al, 2019).
To avoid lithium toxicity, patients should be advised to avoid NSAIDS (ibuprofen, naproxen) and instead use aspirin or acetaminophen for pain. Patients should also remind their other doctors that they are on lithium, especially when diuretics or blood pressure medications are discussed. The most significant contributors to lithium toxicity are NSAIDS and thiazide diuretics, including hydrochlorothiazide (HCTZ) and chlorthalidone. See page 26 for the full list of “battery chargers” that increase lithium levels (ACE inhibitors, ARBs, metronidazole, etc).
Lithium side effects are dose-dependent, including weight gain, fine tremor, acne, excessive thirst, and frequent urination. If thirst and polyuria are extreme, the cause may be lithium-induced nephrogenic diabetes insipidus (deficient response by kidneys to ADH). If nausea is a problem, reduce dose or switch to Lithium ER (Lithobid). Otherwise, immediate release lithium is preferable for maintenance treatment. Taking the entire daily dose of immediate release lithium at bedtime reduces polyuria and decreases the risk of renal problems (Gitlin et al, 2016) by giving the kidneys a break.
Lithium increases the incidence of hypothyroidism 6-fold. Since about 15% of lithium-treated patients will become hypothyroid, TSH should be monitored routinely so levothyroxine (Synthroid) can be added if TSH gets high. Renal function needs to be monitored with a metabolic panel (BMP or CMP). When lithium is combined with a 1st generation antipsychotic, extrapyramidal symptoms (EPS) and neuroleptic malignant syndrome (NMS) may be more likely, which is considered a neurotoxic effect of unknown mechanism. Rarely, lithium may contribute to serotonin syndrome. For individuals over age 50, it is recommended to get an EKG prior to starting (standard-dose) lithium because arrhythmias are possible. Very rarely lithium is associated with intracranial hypertension (pseudotumor cerebri), which presents as headache and ringing in the ears with heartbeats. If untreated, intracranial hypertension can lead to loss of vision.
When taken during the first trimester of pregnancy, lithium poses a low risk (1 in 1,500) of Ebstein's anomaly, a cardiac condition involving the tricuspid valve. Lithium is certainly less teratogenic than valproic acid (Depakote, Depakene) or carbamazepine (Tegretol). Lithium is considered safe for fetal development after the first trimester, but maintaining steady lithium levels during pregnancy and after delivery is challenging. Lithium concentration of fetal blood is equal to that of maternal blood with levels continually decreasing in the first and second trimesters, risking subtherapeutic concentration. Lithium concentration gradually increases in the third trimester and in the postpartum, risking toxicity. If lithium is continued during pregnancy, levels should be checked weekly.
In 2019 the FDA lowered the approved minimum age for lithium from 12 to 7 years.
Lithium works well in combination with valproic acid (Depakote, Depakene), lamotrigine (Lamictal), and second-generation antipsychotics (SGAs).
Compare pharmacy prices for
Lithobid Titration pack of 12.5mg/25mg package (1 qty)
| Costco | 97.18 |
| Medicine Shoppe | 100.31 |
| Rite Aid | 102.10 |
Copyright 2020, CaferMed LLC


Comments
Post a Comment